treatment of recurrent painful neuroma
A 47-year-old male presented with increasing hypersensitivity after traumatic amputation of the left thumb.
Author or contributor: Case courtesy of Mark S. Rekant, M.D.
Philadelphia Hand to Shoulder Center
patient background
Patient information: 47-year-old male
Injury type: Recurrent neuroma
How injury occurred:
Prior ulnar digital nerve neuroma excision with centro-central anastomosis
Other concomitant injuries:
Tinel’s sign over the digital ulnar nerve at base of left thumb stump
The patient was able to return to normal work capacity 17 days after the neuroma resection and nerve capping procedure.
A 47-year-old male presented with increasing hypersensitivity after traumatic amputation of the left thumb. Three years previously, the patient had undergone an ulnar digital nerve neuroma excision with centro-central anastomosis. Now, the patient was forced to work in a modified capacity due to the pain. Upon examination, it was determined that the patient was positive for Tinel’s sign over the digital ulnar nerve at the base of the left thumb stump. There was no sign of infection or damage and the patient retained wrist motion. After discussion of surgical and non-surgical options, the patient elected to proceed with an excision of the recurrent neuroma with nerve cap placement that reduces the recurrence of the painful neuroma.

After adequate anesthesia and standard preparation, the scar from the previous amputation incision was re-incised and the skin flaps were retracted. The ulnar digital nerve neuroma was identified and resected to healthy fascicle nerve endings. In the process, a radial digital nerve neuroma was also identified and resected. Two Axoguard Nerve Caps were attached over the ulnar and radial digital nerve ends, respectively, with 8-0 nylon sutures. The capped nerves were then placed deep in the thenar muscle. Adequate hemostasis was ensured, and the wound was irrigated with saline prior to closing the skin with 4-0 nylon sutures.
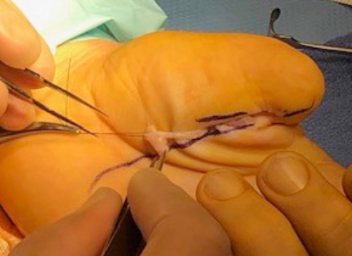
The resection of two digital nerve neuromas, one recurrent, with placement of the Axoguard Nerve Cap was successfully performed. There was no difficulty with placement of the Axoguard Nerve Cap at the resection site of either nerve, and the caps were successfully secured in the thenar muscle. At a 10-day follow-up, there was no sign of infection or drainage, and the sutures were removed. The patient was instructed to perform range of motion exercises. Ultimately, the patient was able to return to normal work capacity 17 days after the neuroma resection and nerve capping procedure.

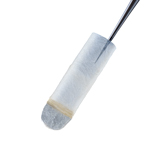
Axoguard Nerve Cap
INDICATIONS FOR USE: Axoguard Nerve Cap is indicated to protect a peripheral nerve end and to separate the nerve from the surrounding environment to reduce the development of symptomatic or painful neuroma.
CONTRAINDICATIONS: Axoguard Nerve Cap is derived from a porcine source and should not be used for patients with known sensitivity to porcine derived materials. Axoguard Nerve Cap is contraindicated for use in any patient for whom soft tissue implants are contraindicated; this includes any pathology that would limit the blood supply and compromise healing, or evidence of a current infection. Axoguard Nerve Cap should not be implanted directly under the skin. Note: This device is not intended for use in vascular applications.




